Research Paper - Women Development in the Bundelkhand Region of Uttar Pradesh by Nagendra Kumar Maurya
Women Development in Bundelkhand Region of Uttar Pradesh
Nagendra Kumar Maurya* & Ankita Pandey**
India is a country of cultural, economic and political diversity. This
diversity provides us a unique opportunity to understand various economic,
political and cultural complexities of our society. Diversity does not mean
inequality among various components of an economy; it means availability of
different alternatives. Steady and sustained growth of an economy requires
inclusive growth of every sector and section of an economy and society. The
growth of different religion, languages, cast, and geographical area should be
balanced in such a way so that no factor can be proved as negative factor and
every section participates in the growth of economy at equal rate. As some areas
have good potential to grow but some areas don’t have such beneits and due to
this they reported low growth, in such condition government requires to pay
special attention on these areas so that they can also participate in economic
growth at equal rate.
A society can be improved only when its contributory parts grow at equal rate.
If any contributing factor gets less facilities and opportunities as compared to
availability of those facilities to others, that section will certainly
contribute at low rate and condition of that section will deteriorate further.
Likewise gender inequality also requires attention by the policy makers. Every
religion, cast and political economy gets contribution from male and female
both. And as our society is male dominated, condition of women could not be
supposed good whether we discuss about their health, education or awareness.
This research paper is an attempt to analyse the level of women development from
the perspective of health and education in Bundelkhand region of Uttar Pradesh.
INTRODUCTION
The mere fact that “women hold up half the sky” does not appear to give women a position of dignity and equality. True that over the years women have made great strides in many areas with notable progress in reducing some gender gap. Yet sprawling inequalities persist in access of women to education, health care, physical & inancial resources and opportunities in economic, social, cultural and political sphere. Gender inequality holds back the growth of individuals, the development of nations and the evolution of societies to the disadvantage of both men and women. Gender issues are not simply talking about women’s issues. Understanding gender means understanding opportunities, constraints and the impact of change as they affect both men and women.
After independence, the Government of India has taken numerous measures to hoist the status of women and to establish gender equality. But women still are one of the most powerless and marginalized sections of Indian society. The 2001 census shows that the sex ratio for India is 933, which is lowest in the world. A declining sex ratio has other consequences for State and societal security. In this research paper an attempt has been made to analyse the level of women development from the perspective of health and education in Bundelkhand region of Uttar Pradesh.
REVIEW OF LITERATURE
There are, however, studies on women development but no, speciically, known studies regarding women development in Bundelkhand region of Uttar Pradesh. It has been found from the various reviews that a focus has to be made on identifying health and education as thrust factors as both has played a very important role in development of women, which in turn indicates a need for studying this area.
* Assistant Professor, Institute of Economics and Finance, Bundelkhand
University, Jhansi
** Teaching Assistant, Institue of Economics and Finance, Bundelkhand
University, Jhansi
According to Singh (1987), if modernity is prerequisite for social, economic and political development, health modernity is the prerequisite for human development, which undoubtedly is the basic prerequisite of all development. The individual must be alive and cognitively competent to be economically productive, socially liberal and politically democratic.
Jafferey (1997) found in her study that unless women are educationally empowered; they can not achieve the goal of political and economic empowerment. Only education can enable women to get or otherwise snatch away the opportunities that the other section of the society specially men enjoy. Without education the hidden values and abilities of women can not be fully realised.
Narula Manju (2009) studied development of elementary education of Bundelkhand region of U.P. and concluded that in spite of various initiatives taken by the government to achieve the goal of UEE (Universal Elementary Education) in Bundelkhand region of U.P. vast disparities were observed in terms of literacy, access, participation, and gender. Kishor and Gupta (2009) in their study found that Children’s likelihood of being fully immunized increases with mothers’ education; but girls beneit more than boys from having a mother who is highly educated.
However, it is evident that the debate on participation of women development is a never ending issue. This paper discusses the development of women of Bundelkhand region of Uttar Pradesh from two main dimensions: health and education.
DATA SOURCE
This research work is based on secondary data. Data has been taken from DLHS-3 (District Level Household and Facility Survey), 2007-08 published by International Institute for Population Sciences (IIPS), Mumbai and from various Uttar Pradesh Government reports. The area of study is conined to Bundelkhand region of Uttar Pradesh. Aggregate analysis at the region level does not provide us a true picture of the district wise variation of the development of women. Therefore a district wise analysis and comparison on the basis of DLHS-3 (2007-08) and DLHS-2 (2002-04) has been made to draw out the conclusions.
DEMOGRAPHIC FEATURES OF BUNDELKHAND REGION
There are four economic regions of U.P. namely (i) Western (ii) Central (iii) Eastern and (iv) Bundelkhand. There are vast inter-regional disparities in respect of development indicators among these four regions. The Eastern and Bundelkhand regions are comparatively more backward as compared to Western and Central regions.
Bundelkhand region is divided between the states of Uttar Pradesh and Madhya Pradesh with larger portion lying in later. It comprises seven districts of Uttar Pradesh i.e. Jhansi, Mahoba, Jalaun, Hamirpur, Chitrakoot, Banda and Lalitpur and six districts of Madhya Pradesh i.e. Datia, Tikamgarh, Chhatarpur, Panna, Damoh and Sagar. Table 1 reveals region-wise economic and demographic features according to 2001 Census.
DISTRICT WISE ANALYSIS OF HEALTH STATUS
The health of women is intrinsically linked to their status in society. Research on women’s status has found that the contributions Indian women make to families often are overlooked, and instead they are viewed as economic burdens. There is a strong son preference in India, as sons are expected to care for parents as they age. This son preference, along with high dowry costs for daughters, sometimes results in the mistreatment of daughters. Further, Indian women have low levels of both education and formal labor force participation.
Table-1, Region - Wise Comparative Status Of Development In U.P.
| SN. | Development Indicator | Eastern | Western | Central | Bundel Khand | U.P. |
| 1 | Population - 2001 (Lakh) | 666.11 | 611.95 | 301.59 | 82.32 | 1661.98 |
| 2 | Area - 2001 (Sq. km.) | 85845 | 79831 | 45834 | 29418 | 240928 |
| 3 | Density of population (per sq.km.) (2001) | 776 | 767 | 658 | 280 | 690 |
| 4 | Decennial growth in population (%) (1991-2001) | 25.58 | 26.55 | 26.29 | 25.57 | 25.91 |
| 5 | Literacy percentage(2001) | 54.27 | 57.36 | 57.58 | 59.30 | 56.27 |
| 6 | Literacy percentage 2001(Female) | 39.13 | 43.96 | 45.52 | 43.11 | 42.22 |
| 7 | Teacher pupil ratio (2004-05) | |||||
| (a) Junior Basic School | 94 | 92 | 95 | 78 | 92 | |
| (b) Senior Basic School | 123 | 114 | 109 | 48 | 111 | |
Source: Annual Plan-2008-09, Vol.-1, State Planning Commission, Uttar Pradesh Government, Uttar Pradesh.
They, typically, have little autonomy, living under the control of irst their fathers, then their husbands, and inally their sons. Finally, a woman’s health affects the household economic well-being, as a woman in poor health will be less productive in the labor force. While women in India face many serious health concerns, this research paper focuses on only four key health issues: marriage and fertility, maternal health, family planning, and knowledge of HIV/AIDS & RTI/STI.
Marriage and Fertility
Health status of women is basically dependent upon their age of marriage. Percentage of girls marrying before completing 18 years have drastically reduced in previous years (see Appendix-3) such as this was 53.3, 62.4 percent for Jhansi and Chitrakoot respectively as per reported by DLHS-2 which went down to 16.5 and 29 percent respectively for the same districts as per DLHS-3. This is a healthy sign for the whole region except Lalitpur where no signiicant decline has been recorded.

Sex ratio at birth for all seven districts is showing a signiicant improvement over previous years. However, unfavorable sex-ratio at higher ages still raising some questions on the society (due to strong son preference) and policy makers (failure for implementing strong law) that why it is low at higher age for both at region as well as district level. On the other hand, signiicant decline has been recorded in the case of child marriage (below 18 years) across the region, but still a long way to go.
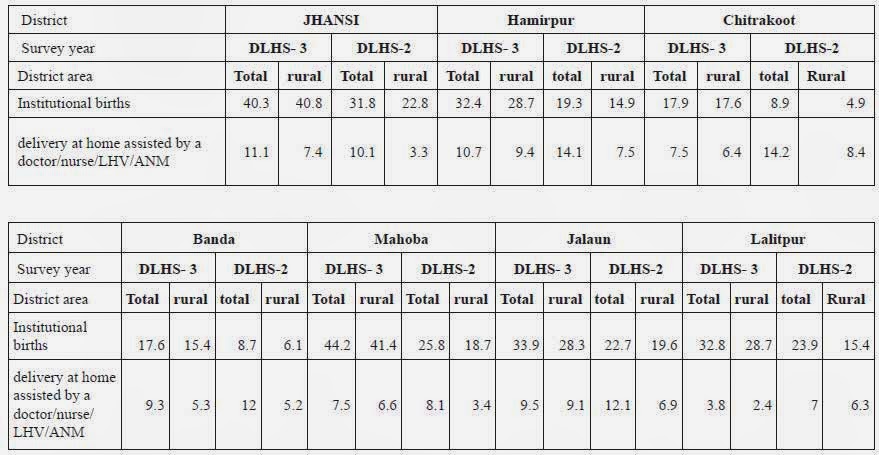
Maternal Health
Graph 2 is explaining the status of maternal health of each district: status of delivery at home assisted by nurse and institutional births. Number of Institutional births is improving in every district of Bundelkhand where Mahoba is best performing district with 44.2 percent as per DLHS-3 as compared to 25.8 percent as per DLHS-2. In case of delivery at home assisted by nurse/doctor, Jhansi, Hamirpur and Jalaun are showing increase in igure while Lalitpur and Banda are showing decline during the same time period. Lalitpur is showing lowest number of deliveries at home. However, Hamirpur and Mahoba are performing well on total basis but in case of rural area, delivery at home is showing increasing trend. (See Appendix-5)

Family Planning
Every district is showing improvement in using family planning method and modern method except Mahoba where there is a decline in preferring any method at total basis but there is an increase in using any modern method at both rural and total basis compared to DLHS-2. Jhansi is a leading district among all showing greater willingness to use family planning method but there are also some surprising facts regarding rural areas of district Jhansi, Hamirpur, Mahoba where rate of preference to use any modern method or any method is greater than urban areas as per DLHS-3.This situation would be better if government make more stringent efforts to fulill unmet demand for family planning for both limiting and spacing purposes. This is evident from the data that there is only marginal improvement in the situation over DLHS-2 for all districts as well as for rural area also.
However, a huge gap has been found in using sterilization as family planning method between male and female. Male dominancy is apparent as women are, mainly, using (probably forcefully) sterilization for limiting purpose i.e. 48.6, 29.9 and 32.8 percent for Jhansi, Hamirpur and Lalitpur respectively, whereas for men these are 0.3, 0.0 and 0.4 percent respectively for the same districts as per DLHS-3. (See Appendix-3)
Knowledge of HIV/AIDs
Prevention is better than cure is well recognized fact. Awareness amongst women about HIV/AIDS could be proved a boon for their health. Data is available separately for married and unmarried women regarding awareness and for other indicators. This classiication is very important for better understanding and policy formulation because more and more youngsters are breaking their virginity in early age and becoming prone to HIV/RTI. By looking at the data (see Appendix-4), it is evident that the percentage of unmarried women heard of HIV/AIDS is more than married women. Compared with DLHS-2 the data are showing improvement in case of married women of all districts except one i.e. Chitrakoot where awareness level was 32.8 percent as per DLHS-2 but this igure went down to 25 percent as per DLHS-3.
However, still people are not ready for testing probably due to hesitation & fear of unacceptability by the family members and society, although, married women are taking the initiatives but still a long way to go in this direction. On the other hand, a social taboo haunting the unmarried one regarding HIV/RTI testing. Knowledge about most commonly prevalent diseases i.e. RTI/STI is not satisfactory (about 10-20 percent) raising more concern about women health for both married and unmarried.
DISTRICT WISE ANALYSIS OF EDUCATION STATUS
If we want to remove discrimination from the society, irst of all we have to educate the people, that enable them to understand their rights and various opportunities prevailing in the economic environment and different health related aspects. Literacy rate of women, as per Census 2001, Bundelkhand region has the second position of Uttar Pradesh. Low level of women literacy compared with male literacy in all districts, is the main reason behind their less development on various issues involving their health concern also.
This is a real fact that society does not want to pay adequate attention on the literacy of women. This may be ascribed to common perceptions prevailing in the society that main objective of a women’s life is to look after home, cooking food, giving birth to children and handling a job of caretaker of whole family. Thus, people do not feel the necessity of education for women as they think education is not essential to fulill all these purposes. Even, they believe that good education would, certainly, bring change in the mind of women hence educated women will challenge the concept of male dominancy in the society.

By looking at facts (Appendix-6), female literacy in Jhansi district is the highest i.e. 60.3 percent as whole and 53.4 percent for rural areas. Backwardness of women is evident from the fact that male literacy is very high in comparison to females; even lowest level of literacy of male (72.3 percent for Chitrakoot) is higher than the highest of female for any districts. However, highest male literacy 84.7 percent on total basis and 83.2 percent in rural area in Jhansi district is not a big achievement; still it requires some signiicant steps for the improvement. Likewise Women literacy lowest in Chitrakoot district on total basis i.e. 47.4 percent while in rural area; it is lowest in Banda district i.e. 43.9 percent requires a special attention from the policy makers.
But the things are improving, percentage of girls (6-11years) attending school is quite good in all districts where Jhansi is showing better picture on total basis (99.6%) as well as 100% in rural area, if we compare it with data of boys (6-11 years) attending schools, Jhansi district is again showing highest percentage 99.7% on total basis and 100% in rural area. The lowest percentage for both girls and boys is in Chitrakoot district with 97.6% and 97.7% respectively.
CONCLUSION
Since, no single district is doing fair in all indicators; some are performing well in some indicators while lagging behind in others, it may be said that scenario of health and education of women in Bundelkhand region is improving but not satisfactory. It is evident that situation of education is better compared with that of their health. People are experiencing and understanding the beneits from education but still they are relatively ignorant about issues related with their health like family planning and knowledge about HIV/ AIDs & RTI/STI.
The reasons may be high cost of routine checkup, less awareness about symptoms, and hesitation to take consultation. More efforts, regarding awareness amongst them on their health, are to be done, so that existing situation can be improved. However, women development is not subject to only health and education status, it consists of social, economic, and political freedom. This paper tries to observe actual level of women development on the basis of health and education status and also to know various possibilities to improve on these issues. Thus things are improving and many plans are running, but there is need to expand and modify their existing plans so that untouched area can be beneitted.
References
Annual Plan-2008-09, Vol.-1, State Planning Commission, Uttar Pradesh Government, Uttar Pradesh.
Dewan Renu, (2008), “Women Empowerment and Health Modernity: a
Socio-Psychological Study of Tribal and Non Tribal in Jharkhand”, Journal of
Economic and Social Development, Ranchi, Jharkhand,
Pg 94-95.
District Level Household and Facility Survey under Reproductive and Child Health Project (DLHS-3) - 2007-08, International Institute of Population Sciences, Mumbai.
Jaffery F., (1997), ‘ Knowledge is power’, One India One People journal, One India One People foundation, Mumbai, Pg 11-12.
Kishor Sunita and Gupta Kamla. 2009. “Gender Equality and Women’s Empowerment
in India”, National Family Health Survey (NFHS-3), International Institute for
Population Sciences; Mumbai, India,
2005-06.
Narula Manju, (2009), “Education, Gender, Access and Participation to Elementary Education in Bundelkhand Region of Uttar Pradesh”, Department of Educational Administration, NUEPA.
Singh Parmar S. B., (1987), “The Rural Hindu Family in Continuity and Change”, Vohra Publishers and Distributors, Allahabad.
The Status of Women- Facts on Inequality and Crimes against Women, SWAYM, 9/2B, Deodar Street, Kolkata-700019.
Velkoff A.Victoria. & Adlakha Arjun, (Dec. 1998), “Women’s Health in India”, Women of the World, International Programs Centre.
APPENDIX-1
Proile of Bundelkhand Region of Uttar Pradesh (Census 2001)
Journal of Economic and Social Development
| district indicators/ districts | Jhansi | Hamirpur | Chitrakoot | Banda | Mahoba | Jalaun | Lalitpur |
| Population ( in thousands) | 1744 | 1043 | 766 | 1537 | 708 | 1454 | 977 |
| Decadal growth rate (1991-01) | 23.23 | 17.85 | 34.33 | 18.49 | 21.8 | 19.39 | 29.98 |
| Sex Ratio (no of females par 1000 males) | 871 | 851 | 873 | 860 | 866 | 849 | 882 |
| Present urban population | 40.79 | 16.65 | 9.99 | 15.87 | 21.86 | 23.41 | 14.52 |
| Present SC population | 28.06 | 22.79 | 26.34 | 20.82 | 25.77 | 27.04 | 24.93 |
| Present ST Population | 0.06 | 0.01 | 0 | 0 | 0.01 | 0.01 | 0 |
| Female Literacy rate ( 7 years and above) | 50.16 | 40.13 | 50.29 | 36.77 | 36.41 | 49.2 | 32.97 |
| Male literacy rate (7 years and above) | 78.76 | 71.86 | 77.69 | 69.28 | 67.74 | 77.39 | 63.81 |
Source:- Data Compiled from DLHS-3 published by IIPS, Mumbai.
APPENDIX-2
Marriage and Fertility
| District | Jhansi | Hamirpur | Chitrakoot | Banda | ||||||||||||
| Survey year | DLHS-3 | DLHS-2 | DLHS-3 | DLHS-2 | DLHS-3 | DLHS-2 | DLHS-3 | DLHS-2 | ||||||||
| District area | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural |
| Percentage of girl marrying before completing 18 years | 16.5 | 17.7 | 53.3 | 70.4 | 20 | 21.4 | 37.6 | 47.8 | 29 | 31.2 | 62.4 | 71.3 | 29 | 31 | 34 | 46.1 |
| Sex ratio at birth | 122 | 105 | 116 | 113 | 104 | 103 | 108 | 111 | ||||||||
| Percentage of births to women during age 15-19 out of total births | 11.3 | 13.3 | 10.1 | 11.1 | 11 | 11.3 | 14.2 | 14.6 | ||||||||
| District | Mahoba | Jalaun | Lalitpur | |||||||||
| Survey year | DLHS - 3 | DLHS -2 | DLHS - 3 | DLHS -2 | DLHS - 3 | DLHS - 2 | ||||||
| District area | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural |
| Percentage of girl marrying before completing 18 years | 27.7 | 30 | 46.7 | 50.3 | 27.7 | 30.3 | 42.8 | 52.7 | 58.9 | 63 | 64 | 75.2 |
| Sex ratio at birth | 120 | 116 | 112 | 110 | 112 | 115 | ||||||
| Percentage of births to women during age 15 19 out of total births | 17 | 18.1 | 8.2 | 9.1 | 11.6 | 12.7 | ||||||
Source:- Data Compiled from DLHS-3 published by IIPS, Mumbai
APPENDIX-3
Family Planning (currently Married women age 15-49, data in Percentage)
| District | Jhansi | Hamirpur | Chitrakoot | Banda | ||||||||||||
| Survey year | DLHS - 3 | DLHS - 2 | DLHS - 3 | DLHS-2 | DLHS- 3 | DLHS-2 | DLHS- 3 | DLHS-2 | ||||||||
| District area | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural |
| Current use: | ||||||||||||||||
| Any method | 65.6 | 66.2 | 55.1 | 53 | 56.6 | 56.8 | 51 | 47.2 | 45.1 | 44.6 | 41.3 | 38.6 | 45.1 | 44.5 | 39.5 | 32.5 |
| Any modern method |
56.5 | 59.2 | 51.1 | 50 | 42.1 | 41.4 | 32 | 29 | 32.5 | 31.7 | 27.7 | 25.4 | 25.8 | 24.9 | 24 | 16.9 |
| female sterilization | 48.6 | 55.8 | 43.7 | 45.7 | 29.9 | 30.7 | 23.2 | 24 | 26.3 | 26.4 | 22 | 22.2 | 18.6 | 19.1 | 13.5 | 11 |
| male sterilization | 0.3 | 0.4 | 0.3 | 0.2 | 0 | 0 | 0.5 | 0.7 | 0.4 | 0.3 | 0 | 0 | 0.3 | 0.4 | 0.2 | 0 |
| IUD | 0.7 | 0 | 0.2 | 0.3 | 0.3 | 0.1 | 0.2 | 0.1 | 0.6 | 0.4 | 1 | 0.5 | 0.4 | 0.3 | 1 | 0 |
| Pill | 1.5 | 0.4 | 1 | 0.7 | 0.6 | 0.7 | 0.8 | 0.7 | 0.8 | 0.5 | 0.7 | 0.4 | 0.4 | 0.3 | 1.4 | 1.4 |
| condom | 5.4 | 2.6 | 6 | 3.1 | 11.2 | 10 | 7.1 | 3.3 | 4.4 | 3.9 | 4 | 2.3 | 6.1 | 4.8 | 8 | 4.5 |
| Unmet need for family planning: | ||||||||||||||||
| Total unmet need | 13.5 | 12.2 | 19.4 | 21 | 23.7 | 24 | 25.2 | 26.1 | 31.4 | 32.5 | 27.4 | 27.9 | 26.9 | 26.8 | 29.8 | 31.7 |
| for spacing | 5.5 | 6.4 | 8.3 | 9.6 | 8.6 | 10 | 10.7 | 11.6 | 11.2 | 12 | 11.2 | 11.5 | 8.1 | 8 | 10.2 | 11.2 |
| for limiting | 8 | 5.8 | 11.1 | 11.4 | 15.1 | 14 | 14.5 | 14.5 | 20.2 | 20 | 16.2 | 16.4 | 18.8 | 18.8 | 19.6 | 20.5 |
|
District |
Mahoba | Jalaun | Lalitpur | |||||||||
| Survey year | DLHS - 3 | DLHS - 2 | DLHS - 3 | DLHS - 2 | DLHS - 3 | DLHS - 2 | ||||||
| District area | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural |
| Current use: | ||||||||||||
| Any method | 52.3 | 53 | 54.8 | 53.4 | 54.7 | 53.8 | 48.2 | 47.6 | 55.5 | 53.6 | 39.9 | 34.1 |
| Any modern method |
44.7 | 45.8 | 38.3 | 37.6 | 46.7 | 46.2 | 38.7 | 37.2 | 42.4 | 41.3 | 29.7 | 23.6 |
| female sterilization | 36.5 | 38.8 | 26.3 | 29.5 | 34.6 | 37.7 | 28.2 | 30.3 | 32.8 | 33.9 | 23.3 | 21 |
| male sterilization | 0.4 | 0.5 | 0.2 | 0.2 | 0.2 | 0.1 | 0 | 0 | 0.4 | 0.5 | 0.4 | 0.2 |
| IUD | 0.2 | 0.3 | 0.5 | 0 | 0.8 | 0.6 | 1.8 | 0.9 | 0 | 0 | 0.4 | 0.1 |
| Pill | 0.5 | 0.4 | 0.6 | 0.5 | 1.3 | 0.8 | 1.7 | 1.4 | 1 | 0.8 | 1.1 | 0.5 |
| condom | 7 | 5.7 | 10.5 | 7.2 | 9.9 | 6.9 | 7 | 4.4 | 8.1 | 6 | 4.3 | 1.7 |
| Unmet need for family planning: | ||||||||||||
| Total unmet need | 22.3 | 22.2 | 21.6 | 22.5 | 21.9 | 22.6 | 23.8 | 23.8 | 20.5 | 21.5 | 33.1 | 34.8 |
| for spacing | 8.1 | 8.6 | 9.5 | 10.1 | 7.5 | 7.6 | 8.1 | 8.4 | 9.2 | 9.9 | 11.5 | 12.5 |
| for limiting | 14.2 | 13.6 | 12.1 | 12.4 | 14.4 | 15 | 15.7 | 15.4 | 11.3 | 11.6 | 21.6 | 22.3 |
Source:- Data Compiled from DLHS-3 published by IIPS, Mumbai.
APPENDIX-4
Knowledge of hiv/aids & rti/ sti among ever Married and unmarried women (%)
| District | Jhansi | Hamirpur | Chitrakoot | Banda | ||||||||||||
| Survey year | DLHS - 3 | DLHS - 2 | DLHS - 3 | DLHS - 2 | DLHS - 3 | DLHS - 2 | DLHS - 3 | DLHS - 2 | ||||||||
| District area | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural | Total | Rural |
| Knowledge of HIV/AIDS & RTI/STI Among Ever Married Women Age 15-49 | ||||||||||||||||
| Women heard of HIV/AIDs | 33.1 | 21 | 28.7 | 13.6 | 35.7 | 33.2 | 29.6 | 19.8 | 25.4 | 22 | 32.8 | 22.6 | 27.2 | 21.2 | 28.4 | 14.3 |
| women who knew that consistent use of condom use can reduce the chances of getting HIV/AIDs | 65.7 | 64.8 | 18 | 12.9 | 36.6 | 30.6 | 38.4 | 37.2 | 41.6 | 41.6 | 25.5 | 20.3 | 26.7 | 23.1 | 16.5 | 16.4 |
| women having correct knowledge of HIV/AIDS | 88.2 | 81.1 | 90 | 90.5 | 93.2 | 92.4 | 84.8 | 81.9 | ||||||||
| women underwent test for detecting HIV/AIDS | 0 | 0 | 2.8 | 1.7 | 1.7 | 1.2 | 1.2 | 1.1 | ||||||||
| Women heard of RTI/STI | 13.5 | 8.5 | 15.6 | 12.1 | 17 | 16.1 | 34.4 | 27.5 | 12.3 | 10.5 | 37.9 | 32.4 | 11.2 | 8 | 34.4 | 29 |
| Knowledge of HIV/AIDS Among Ever Unmarried Women Age 15-24 | ||||||||||||||||
| Women heard of HIV/AIDs | 58.4 | 41.4 | 63.6 | 56.6 | 47.3 | 39.2 | 51.1 | 41.2 | ||||||||
| Women who knew that consistent use of condom use can reduce the chances of getting HIV/AIDs | 58.7 | 56.9 | 37.4 | 29.1 | 33.3 | 31.2 | 31.2 | 33.9 | ||||||||
| Women having correct knowledge of HIV/AIDS | 91 | 85.1 | 92.2 | 93.5 | 93.6 | 93.1 | 88.8 | 88.3 | ||||||||
| Women underwent test for detecting HIV/AIDS | 0 | 0 | 0 | 0 | 0 | 0 | 0.5 | 0 | ||||||||
| Women heard of RTI/STI | 20.8 | 12.2 | 31.7 | 30.9 | 21.4 | 17.7 | 15.3 | 12.7 | ||||||||
Source:- Data Compiled from DLHS-3 published by IIPS, Mumbai
APPENDIX-5
Knowledge of hiv/aids & rti/sti among ever Married and unmarried women (%)

APPENDIX-6
Maternal Health (%)
APPENDIX-7
Literacy Level

Nagendra Kumar Maurya (Contact Author)
Aliganj
Lucknow, Uttar Pradesh 226024
India
05222325021 (Phone)
Courtesy: SSRN
- Anonymous's blog
- Log in to post comments